A post by Pat
****CLARIFICATION on Worse than dead state
Based on a couple of comments below, let me clarify that having a negative QALY score does not necessarily mean the patient is in a Terri Schiavo vegetative state or something equivalently dire. There was a controversy covered in the British news last year over how NICE does their calculations. The formula is super secret. A public advisory group with the bizarre title The Citizens Council of NICE convened to discuss whether or not NICE had to update their formula. One wheelchair-bound member of the group was surprised to find out she rated a negative QALY score.
NHS drugs body Nice reviews drug funding
The Citizens Council of Nice, a representative sample of 30 members of the public, examined the calculations earlier this year and recommended “a thoughtful and penetrating review”.
Nice’s method involves quality of life scores which one Citizens Council member found would give her a negative score meaning she would be ‘better off dead’ as she is confined to a wheelchair, a report of the meeting said.
The news report says the NHS budget has no bearing on the calculations. That’s absurd. Cost is the entire purpose for the calculation. The premise underlying QALY is how much is a year of your life worth in terms of other people’s money not the quality of your life to you and your loved ones.
******
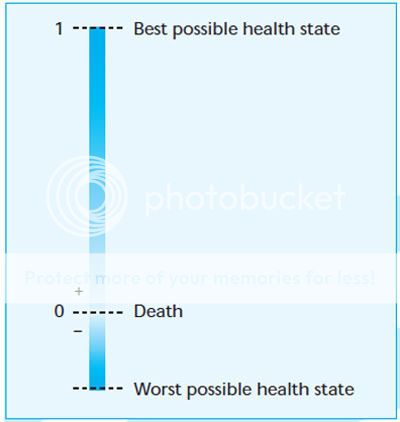
This chart indicates the range of possible QALY scores. QALY stands for quality adjusted life year—a year of life adjusted for its quality or its value—a mathematically derived value ranging from plus one to negative scores. The formula is used by the U.K.’s National Institute of Clinical Excellence, a.k.a., NICE, as a guideline for NHS treatment. Many people think it’s not so nice. This is a lottery for your life. NICE evaluates which drugs, devices and procedures are economical and to whom they are worth giving.
A quality-adjusted life year (QALY) takes into account both quantity and the quality of life generated by healthcare interventions. It is the arithmetic product of life expectancy and a measure of the quality of the remaining life years. l A QALY places a weight on time in different health states. A year of perfect health is worth 1; however, a year of less than perfect health life expectancy is worth less than 1. Death is considered to be equivalent to 0, however, some health states may be considered worse than death and have negative scores.
QALYs provide a common currency to assess the extent of the benefits gained from a variety of interventions in terms of health-related quality of life and survival for the patient. When combined with the costs of providing the interventions, cost-utility ratios result; these indicate the additional costs required to generate a year of perfect health (one QALY). Comparisons can be made between interventions, and priorities can be established based on those interventions that are relatively inexpensive (low cost per QALY) and those that are relatively expensive (high cost per QALY).
If that sounds like something you wouldn’t like here, consider this. One of the stealth bombs in the stimulus bill that hasn’t gotten much attention is $1.1 billion for “comparative effectiveness research” [CER].
The wording is carefully chosen in the legislation, referring to clinical research effectiveness. That is effectiveness analysis of drugs and treatments compared to other drugs and treatments. No mention of QALY or cost effectiveness because politicians and insurance companies know there will be a negative impact in introducing the value of life factor into the mix—at this point. NICE is often cited by proponents of CER as a model. It sounds like a reasonable utility to control costs by identifying efficiencies. You know this isn’t going to be temporary. If you think establishing a federal bureaucracy like this is a wholly beneficial exercise that will not evolve into rationing as government takes over the healthcare system, you’re betting your life on it.
A Comparative Effectiveness Research Institute has been on the Democrat wish list for some time. Last August Max Baucus and Kent Conrad introduced legislation to establish such an institute. Obama supports the idea.
In 2007 the CBO did a study on comparative effectiveness of medical treatments with respect to Medicare and Medicade.
Because any private-sector entity (such as a health plan) has only a limited incentive to produce or pay for information that could benefit many entities- including its competitors-an argument can be made for a larger federal role in coordinating and funding research on comparative effectiveness. In addition, because federal health insurance programs play such a large role in financing medical care and account for such a large share of the budget, the federal government itself has an interest in generating evaluations of the effectiveness of different approaches to health care.
This is what is in the stimulus bill:
S. 336 – American Recovery and Reinvestment Act of 2009
Agency for Healthcare Research and Quality (AHRQ)
• $1.1 billion for comparative clinical effectiveness research.
o $300 million shall be administered by the Agency for Healthcare Research and
Quality;
o $400 million shall be transferred to the National Institutes of Health (NIH); and
o $400 million shall be allocated at the discretion of the Secretary of Health and
Human Services.The use of “clinical†is important because the language would not appear to allow the use of cost effectiveness as a criterion in the research.
When the government pays the bills for healthcare, there will eventually be rationing. Innovation in pharmaceutical products will be stifled. The ultimate question is where is this leading when you’re number comes up negative and the government decides you’re not worth keeping alive?



Egads! It just keeps getting uglier and uglier.
With the dozens of reasons not to have socialized medicine, this is the one that is impossible to refute:
No matter how evil, greedy, corrupt your private insurance company is, it is in their best interests to keep you alive (If you’re dead, you can’t pay premiums.)
No matter how benevolent, comapassionate, tolerant the government health insurance providers are, it is in their best interests for you to die. (One less body to finance.)
Tammy,
From Bloomberg News….
With all the money pledged to “fix” this “recession”…. we could have paid off more than 90% of the MORTGAGES IN THE ENTIRE COUNTRY….
this does not include the “guarantee” given to fannie/freddie….
This fact is utterly shocking….and despicable
Article:
http://www.bloomberg.com/apps/news?pid=20601087&sid=aGq2B3XeGKok&refer=home
Hideous. They even used the same acronym. How’s that for life imitating art?
The underlying fact, which cannot be openly discussed by politicians, is that health care, like every other commodity, is a finite resource. So you take your choice, either it’s allocated by market forces, or rationed by the government. Either approach is problematic. I favor the free market, not because it’s a panacea, but because it’s so much better than a monstrous bureaucracy. The free market is flexible and organic; it changes as the world changes, driving down prices and allocating resources with maximum efficiency. Are we going to give that up in favor of authoritarian allocation? Do you really trust the government to take care of you? Go stand in line at the Post Office or the DMV, and then tell me you want that to be your only path to health care.
Consider the hot-button question of abortions. I think we can more-or-less coexist with a government hands-off approach…that is, the government doesn’t outlaw abortions, but neither does it perform them. But when the government monopolizes health care, then one side wins and the “truce” ends. Either there are no abortions, or the government gives abortions as a matter of policy. Government is a one-size-fits-all solution, and one size doesn’t fit all, and any attempt to make one size fits all makes us miserable.
By the way, I do personally believe that some states of health are worse than death. For example, I’d rather be dead than in a Terry Schiavo situation. And I certainly wouldn’t expect the taxpayers to maintain me for decades in a vegetative state. My legal paperwork reflects my attitude. But I make these decisions for myself; I don’t trust the government decision-making process.
Thank you for this post, Pat.
Perhaps it can now be said that the Obama administration & supporters in the House view death as an economic stimulus.
Interesting that Terri Schiavo’s name was brought up. What we witnessed in 2005 with her forced death is what may well become common practice for many like her or those who are elderly, feeble, sick, costly to maintain or – in the eyes of government – worthless and a drain. We will all be subject to federal criteria based on what we do for government as a means for our survival. I don’t recall that being in our founding documents at all.
There are two books I’m going to recommend to everyone. The first is a book I read in 1980 when I was 14, and it changed my life. It’s ‘Whatever Happened to the Human Race?’ by Francis Schafer & Dr. C. Everett Coop (who later became Surgeon General under Reagan). The next is more recent (2001), ‘Culture of Death: The Assault on Medical Ethics in America’ by Wesley J. Smith.
What gives me chills is the fact that I am witnessing events I read about in ‘Whatever Happened…’ nearly 30 years ago unfold in my lifetime! We have entered a point where the government will preach death as a message of duty starting with our aged citizens. Who will be next?
We have been on this path for a while. It simply takes an outrageous act to become normalized through repetition and media manipulation before it becomes acceptable in society. Where it took sometimes years to seduce the public, our information highway has made that process much quicker and easier.
We are truly entering a very dark time in our history.